Laparoscopic bariatric Surgery

Bariatric surgical procedures cause weight loss by restricting the amount of food the stomach can hold, causing malabsorption of nutrients, or by a combination of both gastric restriction and malabsorption. Bariatric procedures also often cause hormonal changes. Most weight loss surgeries today are performed using minimally invasive techniques (laparoscopic surgery).
The most common bariatric surgery procedures are gastric bypass, sleeve gastrectomy, adjustable gastric band, and biliopancreatic diversion with duodenal switch. Each surgery has its own advantages and disadvantages.





Gastric bypass
The Roux-en-Y Gastric Bypass – often called gastric bypass – is considered the ‘gold standard’ of weight loss surgery and is the most commonly performed bariatric procedure worldwide.
The Procedure.
There are two components to the procedure. First, a small stomach pouch, approximately one ounce or 30 milliliters in volume, is created by dividing the top of the stomach from the rest of the stomach. Next, the first portion of the small intestine is divided, and the bottom end of the divided small intestine is brought up and connected to the newly created small stomach pouch. The procedure is completed by connecting the top portion of the divided small intestine to the small intestine further down so that the stomach acids and digestive enzymes from the bypassed stomach and first portion of small intestine will eventually mix with the food.
The gastric bypass works by several mechanisms. First, similar to most bariatric procedures, the newly created stomach pouch is considerably smaller and facilitates significantly smaller meals, which translates into less calories consumed. Additionally, because there is less digestion of food by the smaller stomach pouch, and there is a segment of small intestine that would normally absorb calories as well as nutrients that no longer has food going through it, there is probably to some degree less absorption of calories and nutrients.
Most importantly, the rerouting of the food stream produces changes in gut hormones that promote satiety, suppress hunger, and reverse one of the primary mechanisms by which obesity induces type 2 diabetes.
Advantages.
- Produces significant long-term weight loss (60 to 80 percent excess weight loss)
- Restricts the amount of food that can be consumed
- May lead to conditions that increase energy expenditure
- Produces favorable changes in gut hormones that reduce appetite and enhance satiety
- Typical maintenance of >50% excess weight loss
Disadvantages.
- Is technically a more complex operation than the AGB or LSG and potentially could result in greater complication rates
- Can lead to long-term vitamin/mineral deficiencies particularly deficits in vitamin B12, iron, calcium, and folate
- Generally has a longer hospital stay than the AGB
- Requires adherence to dietary recommendations, life-long vitamin/mineral supplementation, and follow-up compliance
Sleeve gastrectomy
The Laparoscopic Sleeve Gastrectomy – often called the sleeve – is performed by removing approximately 80 percent of the stomach. The remaining stomach is a tubular pouch that resembles a banana.
The Procedure.
This procedure works by several mechanisms. First, the new stomach pouch holds a considerably smaller volume than the normal stomach and helps to significantly reduce the amount of food (and thus calories) that can be consumed. The greater impact, however, seems to be the effect the surgery has on gut hormones that impact a number of factors including hunger, satiety, and blood sugar control.
Short term studies show that the sleeve is as effective as the roux-en-Y gastric bypass in terms of weight loss and improvement or remission of diabetes. There is also evidence that suggest the sleeve, similar to the gastric bypass, is effective in improving type 2 diabetes independent of the weight loss. The complication rates of the sleeve fall between those of the adjustable gastric band and the roux-en-y gastric bypass.
Advantages.
- Restricts the amount of food the stomach can hold
- Induces rapid and significant weight loss that comparative studies find similar to that of the Roux-en-Y gastric bypass. Weight loss of >50% for 3-5+ year data, and weight loss comparable to that of the bypass with maintenance of >50%
- Requires no foreign objects (AGB), and no bypass or re-routing of the food stream (RYGB)
- Involves a relatively short hospital stay of approximately 2 days
- Causes favorable changes in gut hormones that suppress hunger, reduce appetite and improve satiety
Disadvantages.
- Is a non-reversible procedure
- Has the potential for long-term vitamin deficiencies
- Has a higher early complication rate than the AGB



Adjustable Gastric Band
The Adjustable Gastric Band – often called the band – involves an inflatable band that is placed around the upper portion of the stomach, creating a small stomach pouch above the band, and the rest of the stomach below the band
The Procedure.
The common explanation of how this device works is that with the smaller stomach pouch, eating just a small amount of food will satisfy hunger and promote the feeling of fullness. The feeling of fullness depends upon the size of the opening between the pouch and the remainder of the stomach created by the gastric band. The size of the stomach opening can be adjusted by filling the band with sterile saline, which is injected through a port placed under the skin.
Reducing the size of the opening is done gradually over time with repeated adjustments or “fills.” The notion that the band is a restrictive procedure (works by restricting how much food can be consumed per meal and by restricting the emptying of the food through the band) has been challenged by studies that show the food passes rather quickly through the band, and that absence of hunger or feeling of being satisfied was not related to food remaining in the pouch above the band. What is known is that there is no malabsorption; the food is digested and absorbed as it would be normally.
The clinical impact of the band seems to be that it reduces hunger, which helps the patients to decrease the amount of calories that are consumed.
Advantages.
- Reduce the amount of food the stomach can hold
- Induces excess weight loss of approximately 40 – 50 percent
- 3. Involves no cutting of the stomach or rerouting of the intestines
- Requires a shorter hospital stay, usually less than 24 hours, with some centers discharging the patient the same day as surgery
- Is reversible and adjustable
- Has the lowest rate of early postoperative complications and mortality among the approved bariatric procedures
- Has the lowest risk for vitamin/mineral deficiencies
Disadvantages.
- Slower and less early weight loss than other surgical procedures
- Greater percentage of patients failing to lose at least 50 percent of excess body weight compared to the other surgeries commonly performed
- Requires a foreign device to remain in the body
- Can result in possible band slippage or band erosion into the stomach in a small percentage of patients
- Can have mechanical problems with the band, tube or port in a small percentage of patients
- Can result in dilation of the esophagus if the patient overeats
- Requires strict adherence to the postoperative diet and to postoperative follow-up visits
- Highest rate of re-operation
Biliopancreatic Diversion with Duodenal Switch (BPD/DS) Gastric Bypass
The Biliopancreatic Diversion with Duodenal Switch abbreviated as BPD/DS is a procedure with two components. First, a smaller, tubular stomach pouch is created by removing a portion of the stomach, very similar to the sleeve gastrectomy. Next, a large portion of the small intestine is bypassed.
The Procedure.
The duodenum, or the first portion of the small intestine, is divided just past the outlet of the stomach. A segment of the distal (last portion) small intestine is then brought up and connected to the outlet of the newly created stomach, so that when the patient eats, the food goes through a newly created tubular stomach pouch and empties directly into the last segment of the small intestine. Roughly three-fourths of the small intestine is bypassed by the food stream.
The bypassed small intestine, which carries the bile and pancreatic enzymes that are necessary for the breakdown and absorption of protein and fat, is reconnected to the last portion of the small intestine so that they can eventually mix with the food stream. Similar to the other surgeries described above, the BPD/DS initially helps to reduce the amount of food that is consumed; however, over time this effect lessens and patients are able to eventually consume near “normal” amounts of food. Unlike the other procedures, there is a significant amount of small bowel that is bypassed by the food stream.
Additionally, the food does not mix with the bile and pancreatic enzymes until very far down the small intestine. This results in a significant decrease in the absorption of calories and nutrients (particularly protein and fat) as well as nutrients and vitamins dependent on fat for absorption (fat soluble vitamins and nutrients). Lastly, the BPD/DS, similar to the gastric bypass and sleeve gastrectomy, affects guts hormones in a manner that impacts hunger and satiety as well as blood sugar control. The BPD/DS is considered to be the most effective surgery for the treatment of diabetes among those that are described here.
Advantages.
- Results in greater weight loss than RYGB, LSG, or AGB, i.e. 60 – 70% percent excess weight loss or greater, at 5 year follow up
- Allows patients to eventually eat near “normal” meals
- Reduces the absorption of fat by 70 percent or more
- Causes favorable changes in gut hormones to reduce appetite and improve satiety
- Is the most effective against diabetes compared to RYGB, LSG, and AGB
Disadvantages.
- Has higher complication rates and risk for mortality than the AGB, LSG, and RYGB
- Requires a longer hospital stay than the AGB or LSG
- Has a greater potential to cause protein deficiencies and long-term deficiencies in a number of vitamin and minerals, i.e. iron, calcium, zinc, fat-soluble vitamins such as vitamin D
- Compliance with follow-up visits and care and strict adherence to dietary and vitamin supplementation guidelines are critical to avoiding serious complications from protein and certain vitamin deficiencies
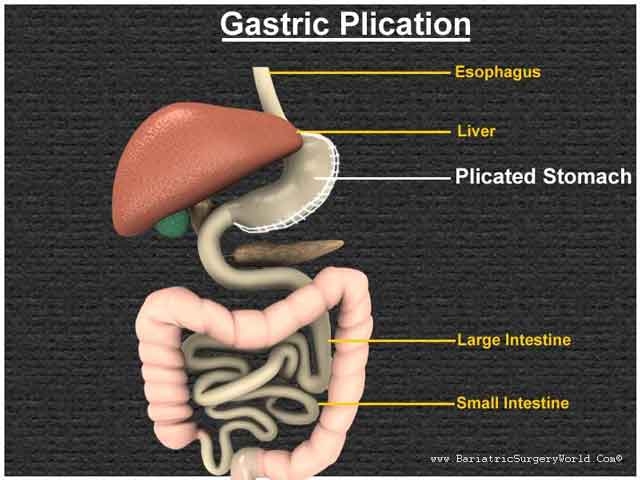
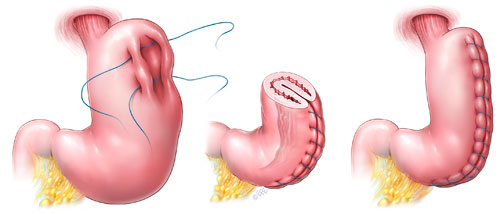
Laparoscopic Gastric Plication
There are several types of bariatric (surgical weight loss) procedures. Some procedures like laparoscopic gastric bypass and laparoscopic sleeve gastrectomy restrict the amount of food that can be eaten at one time and others bypass segments of the intestines to limit the absorption of calories like Roux-en-y gastric bypass. Laparoscopic Gastric Plication is a restrictive procedure that reduces the size of the stomach and limits food intake. This procedure is also referred to as Laparoscopic Greater Curvature Plication (LGCP).
How Is Gastric Plication Performed?
We perform the Gastric Plication as a laparoscopic procedure. This involves making five or six small incisions in the abdomen and performing the procedure using a video camera (laparoscope) and long instruments that are placed through these small incisions.
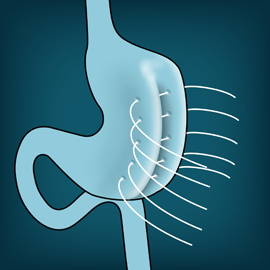
Laparoscopic Gastric Plication, involves sewing one or more large folds in your stomach. During the Laparoscopic Gastric Plication the stomach volume is reduced about 70% which makes the stomach able to hold less and may help you eat less. There is no cutting, stapling, or removal of the stomach or intestines during the Gastric Plicaiton. The Gastric Plication may potentially be reversed or converted to another procedure if needed.
The Gastric Plication procedure is minimally invasive and takes approximately one to two hours to complete. Most patients stay in the hospital for 1-2 days after the procedure.
How Does Gastric Plication Cause Weight Loss?
Gastric Plication is a restrictive procedure. It greatly reduces the size of your stomach and limits the amount of food that can be eaten at one time. It does not cause decreased absorption of nutrients or bypass your intestines. After eating a small amount of food, you will feel full very quickly and continue to feel full for several hours. Gastric Plication may also cause a decrease in appetite.
What Are The benefits Of Laparoscopic Gastric Plication?
Depending on their pre-operative weight, patients can expect to lose between 40% to 70% of their excess body weight in the first year after surgery. Many obesity-related comorbidities improve or resolve after bariatric surgery. Diabetes, hypertension, obstructive sleep apnea and abnormal cholesterol levels are improved in more than 75% of patients undergoing a bariatric procedure. Though long-term studies are not yet available, the weight loss that occurs after Gastric Plication results in significant improvement in these medical conditions in the first year after surgery.
Who is a candidate for Laparoscopic Gastric Plication?
The Laparoscopic Gastric Plication procedure is relatively new, and considered investigational as a primary procedure for weight loss. The Gastric Plication is being offered to patients at the Cleveland Clinic as part of a clinical trial that will better define short and long-term benefits of the procedure. Currently, insurance companies do not cover the Gastric Plication Procedure. Therefore, patients are required to self-pay for the procedure. A financial coordinator from the Bariatric and Metabolic Institute will be available to discuss payment options with you.
What Are The Risks Of Laparoscopic Gastric Plication?
There are risks that are common to any laparoscopic procedure such as bleeding, infection, injury to other organs, or the need to convert to an open procedure. There is also a small risk of a leak from the suture line used to imbricate/plicate (“fold”) the stomach. These problems are rare and major complications occur less than 1% of the time.
Is Laparoscopic Gastric Plication A Good Choice For Me?
Your surgeon may talk to you about Gastric Plication as an option if you have a BMI over 27 with one or more significant co-morbid medical conditions which are generally expected to be improved, reversed, or resolved by weight loss. You should discuss all of the available surgical procedures with your surgeon and determine which procedure is best for you.
Persian International Health Tourism is a private company act as a facilitator between patients/visitors, best medical teams and various hospitals suggesting best available options based on your required treatment or other services.